Unit 1 – Lower medial shin pain in a marathon runner (Free Preview)
Quiz: When you have completed the learning requirements for this unit, you will be able to access its quiz by clicking on the link found at the bottom of this web page. You can attempt the quiz as many times as you need to achieve a pass mark of at least 60%.
Disclaimer: Please read the Disclaimer at the bottom of this page.
Copyright © Educom Pty Ltd: All material on this website (including the text, graphics, videos and downloadable files) are owned by or licensed to Educom Pty Ltd and is subject to copyright and other intellectual property rights under international conventions.
Unit Credit: 2 Hours
How to Complete This Unit
The credit hours for this unit are allocated for progressing through the reading material, answering the questions posed, considering the reflection points, watching the videos, and completing the quiz. When you have completed the learning material in this unit, you will be able to access its multiple-choice quiz by clicking on the link found at the bottom of this web page. You can attempt the quiz as many times as you need to achieve a pass mark of at least 60%.

Content Links
The following buttons can be used to navigate the content in this unit.
How to Complete the Case Scenario Case Structure – The case scenario in this unit is divided into several components. Each component has one or more questions followed by suggested answers.
Our Recommendation – To help you sharpen your clinical reasoning and diagnostic skills, we recommend the following approach: Click the “Hide All Suggested Answers” button below. Read through the first patient case scenario component and answer the question (or questions) posed. When you are ready, click to open the “View Suggested Answer” for that component, read the answer we have provided, and compare it with your own answer. Continue the same approach for the remainder of the case. If you prefer to have all of the “Suggested Answers” visible, click on the “Open All Suggested Answers” button below. You could also hide and open each “Suggested Answer” section individually as you proceed through the case scenario.
![]()
Your Feedback – Your insights can shape the design of our future courses. Whether it’s about the format, structure, or content, your input can help us tailor our courses to better meet your needs. Don’t hesitate to share your thoughts and suggestions. Please contact us if you have any questions.
Patient’s History
In the sections below, you are provided with case history information. The material presents a systematic approach to performing a focused and relevant case history in order to narrow down the possible causes for the patient’s complaint. As you read the following material, you are encouraged to answer the questions posed to test your clinical reasoning and diagnostic skills.
Who is the patient and where is the pain?
When was the onset and what caused the onset?
Your patient is a 30-year-old university lecturer who presents with a primary complaint of right lower leg pain. He points to the lower two-thirds of the medial tibial border as the site of his pain. He believes it is related to running which he began about 6 months ago when he decided to train for his first marathon. The pain has gradually developed over the last 3 months and appears to have coincided with an increase in his running distance.
Question: Based on the information above, what conditions do you think need to be considered?
View Suggested Answer
The patient’s history indicates a chronic condition. His description of lower leg pain can indicate the possibility of several conditions, including:
- Medial lower leg muscle strain
- Tibial stress fracture
- Medial Tibial Stress Syndrome
- Chronic Exertional Compartment Syndrome
- Foot or ankle joint dysfunction or abnormal biomechanics
What are the pain characteristics?
What are the aggravating and relieving factors?
What has been the course of the pain?
He describes his pain as a diffuse ache and rates it as a 7 out of 10 in intensity at its worst. He finds that the pain is aggravated when running and gradually subsides over several hours with rest. He says that the pain has definitely worsened with increases in his running distance over time. He now finds that even simple daily activities like walking and climbing stairs are painful.
Question: How have the pain characteristics, aggravating and relieving factors, and the course of pain influenced your understanding of the possible underlying mechanism?
View Suggested Answer
An aching type of pain that is aggravated by activity and relieved by rest suggests a mechanical cause. The increasing severity and persistence of the pain indicate a worsening of the condition. That his leg pain takes several hours to ease off after running suggests the presence of Medial Tibial Stress Syndrome.
Chronic Exertional Compartment Syndrome is less likely to be present since the leg pain in this condition typically disappears within 10 to 20 minutes after the activity has ended.
Are there any associated symptoms?
He says that he does not experience any associated symptoms such as numbness and tingling.
Question: What does this information indicate?
View Suggested Answer
The absence of associated tingling or numbness helps in ruling out Chronic Exertional Compartment Syndrome.
Is there a past history that is relevant to the current complaint?
He has no previous history of a similar complaint. He reports that he suffered a right ankle sprain in his early twenties.
Question: What does the patient’s past history indicate?
View Suggested Answer
That he has no previous history of a similar complaint suggests that this is a new condition with a strong link to his running. His previous ankle sprain strengthens the possibility of a persistent ankle joint dysfunction, either causing or contributing to his current complaint.
Are there any “red flags”?
The patient is asked the following questions in order to identify any “red flags” that could indicate serious pathology. Even if the patient has already provided information in the case history that relates to these questions, it is recommended that they are readdressed to ensure a thorough exploration.
• Do your pain disappear even for a short time? “Yes, it gradually disappears with rest after I finish a run.”
• Does the pain wake you up at night? “No.”
• Do you feel weak in your legs? “No.”
• Have you recently had any fever, chills, or night sweats? “No.”
• Have you recently had an infection or other illness? “No.”
• Do you have a history of cancer, inflammatory arthritis, or fracture arising from minor trauma? “No.”
Question: Do any of the patient’s responses raise a red flag?
View Suggested Answer
None of the patient’s responses raise a red flag.
What is the list of possible causes for the patient’s complaint?
Question: Based on the information from the case history, what conditions would you include in your differential diagnosis list?
View Suggested Answer
- Medial Tibial Stress Syndrome
- Tibial stress fracture
- Chronic ankle syndesmotic dysfunction
- Medial lower leg muscle strain
- Chronic Exertional Compartment Syndrome
Reflection Point
Please stop and take a moment to consider whether the main requirements of an adequate and relevant patient history taking have been fulfilled. Are there any additional questions you would have asked and, if so, why?
Before the physical examination findings are presented below, please reflect on what physical examination procedures you would perform to adequately evaluate this patient.
Performing Physical Examination
In the sections below, you are provided with physical examination findings for this patient. The material presents a systematic approach to performing a focused and relevant physical examination in order to narrow down the possible causes of the patient’s complaint. As you read the following material, you are encouraged to answer the questions posed to test your clinical reasoning and diagnostic skills. As you read the following material, you are encouraged to identify whether the essential elements of the physical examination have been adequately covered.
Vital Signs
His vital signs are within normal limits.
Inspection
Inspection of the right lower leg is unremarkable with no evidence of swelling or erythaema while inspection of his feet and ankles reveals bilateral pes planus.
Question: What do these findings indicate?
View Suggested Answer
The absence of swelling or erythema is further confirmation that Chronic Exertional Compartment Syndrome is unlikely to be present. The presence of pes planus indicates the possibility of foot or ankle biomechanical disturbance as a contributing factor to his condition.
Range of Motion
Assessment of his ankle and knee range of motion is unremarkable.
Question: What do the range of motion findings indicate?
View Suggested Answer
The results of the range of motion assessment help to rule out ankle and knee joint involvement.
Palpation
There is diffuse tenderness along the distal two-thirds of the posteromedial tibial border. There is no evidence of increased tension in the anterior compartment of the leg. Normal dorsalis pedis and posterior tibial pulses are present. A functional assessment of the foot and ankle joints reveals no abnormalities.
Question: What do the palpation findings indicate?
View Suggested Answer
The diffuse tenderness along the tibia is consistent with the diagnosis of Medial Tibial Stress Syndrome (a stress fracture typically presents as focal tenderness). The lack of tension within the anterior compartment helps to confirm that Chronic Exertional Compartment Syndrome is not present. Normal foot pulses indicate that the patient’s condition is not interfering with blood flow. The normal findings for the foot and ankle functional assessment reduce the likelihood of their biomechanical disturbance as a contributing or causative factor.
Reflection Point
Given the patient’s history and examination findings up until this point, please stop and take a moment to consider which special tests should be performed to further evaluate the patient.
Special Tests
The External Rotation Stress test is performed and is found to be negative with no reproduction of the patient’s pain or evidence of joint instability.
Question: What does the above finding suggest?
View Suggested Answer
This test is designed to detect the involvement of ankle syndesmosis. The negative result helps to rule out dysfunction of this joint as a cause or contributing factor for the patient’s condition. Please watch the video below if you wish to see how the External Rotation Stress test is performed.
The Heel Tap test is performed and is found to be negative.
Question: What does the above finding suggest?
View Suggested Answer
The Heel Tap test is designed to detect the presence of a fracture in the lower extremity. The negative result in this patient indicates the absence of a fracture. Please watch the video below if you wish to see how the Heel Tap test is performed.
The Ankle Anterior Drawer and the Talar Tilt tests are performed and are found to be negative with normal stability present.
Question: What do the above findings suggest?
View Suggested Answer
The Ankle Anterior Drawer and Talar Tilt tests are designed to detect ankle instability. The negative results in this case help to rule out ankle instability as a cause or contributing factor. Please watch the video below if you wish to see how the Ankle Anterior Drawer and Talar Tilt tests are performed.
Reflection Point
Please stop and take a moment to consider whether all the elements of an adequate and relevant physical examination have been completed for this patient. Are there any additional procedures you would have performed and, if so, why?
Clinical Diagnosis
Question: Based on the information you have been provided for this case, what is the most likely clinical diagnosis?
View Suggested Answer
Medial Tibial Stress Syndrome.
Diagnostic Features
Medial Tibial Stress Syndrome
Introduction
Medial Tibial Stress Syndrome (MTSS), often referred to as “shin splints”, causes pain along the distal two-thirds of the medial tibial border. It is a common injury affecting athletes involved in running sports. Health practitioners need to differentiate MTSS from stress fractures and, more importantly, from Chronic Exertional Compartment Syndrome. Another lower leg syndrome of great importance is Acute Compartment Syndrome which is typically caused by local trauma (e.g., fracture of the tibia) resulting in acute loss of blood flow, constituting a medical emergency.
The pathophysiology of MTSS is thought to be a traumatic periostitis of the tibia involving the tendinous attachments of the soleus (primarily), flexor digitorum longus, and posterior tibialis, with tearing of Sharpey’s fibres at their bony insertion.
A number of risk factors may contribute to the development of MTSS. These include:
- Obesity
- Female gender
- Excessive pronation
- Muscle dysfunction
- Incorrect footwear
- Running on hard or uneven surfaces
- Significant increase in running distance
- Fatigue
- History of previous tibial stress fractures
- Vitamin D deficiency and lower bone mineral density
- Leg length deficiency
History and Presentation
- Exercise-induced diffuse pain along the distal two-thirds of the medial tibial border
- Pain is exacerbated by physical activity and typically takes several hours to ease off after the activity and may even persist at rest
- Absence of leg muscle tenseness, cramping, burning pain and numbness/tingling in the foot
Physical Examination
- Diffuse tenderness along the distal two-thirds of the posteromedial tibial border (focal tenderness should alert the examiner to the possibility of a stress fracture)
- Absence of tenseness in the leg compartments (compartment tenseness is a feature of Acute or Chronic Exertional Compartment Syndrome)
- Normal distal pulses and an absence of severe swelling, erythema, or numbness
Imaging and Electrodiagnostic Testing
Medial Tibial Stress Syndrome is usually a clinical diagnosis with imaging typically used to help rule out other conditions. However, if diagnostic imaging is to be used MRI is considered the most sensitive modality. To rule out stress fractures, plain radiography is considered to have poor sensitivity while MRI is considered to be the most sensitive modality for detecting stress fractures.
Red Flags
The following are examples of “red flags” for patients presenting with leg pain:
- History of a significant injury
- Severe or focal pain
- Unrelenting pain
- Nocturnal pain
- Unexplained weight loss
- Fever
- Deformity
- Significant swelling
- Leg pain arising after a prolonged period of immobility or bed rest.
- Presence of tingling, numbness, burning or other neurological impairment
- Loss of distal leg pulses
- Significant loss of range of motion
- Severe tenderness on palpation or severe pain with any examination procedure
If any “red flags” are identified during history taking and clinical examination, referral for urgent medical evaluation and further investigation is warranted.
For Patients
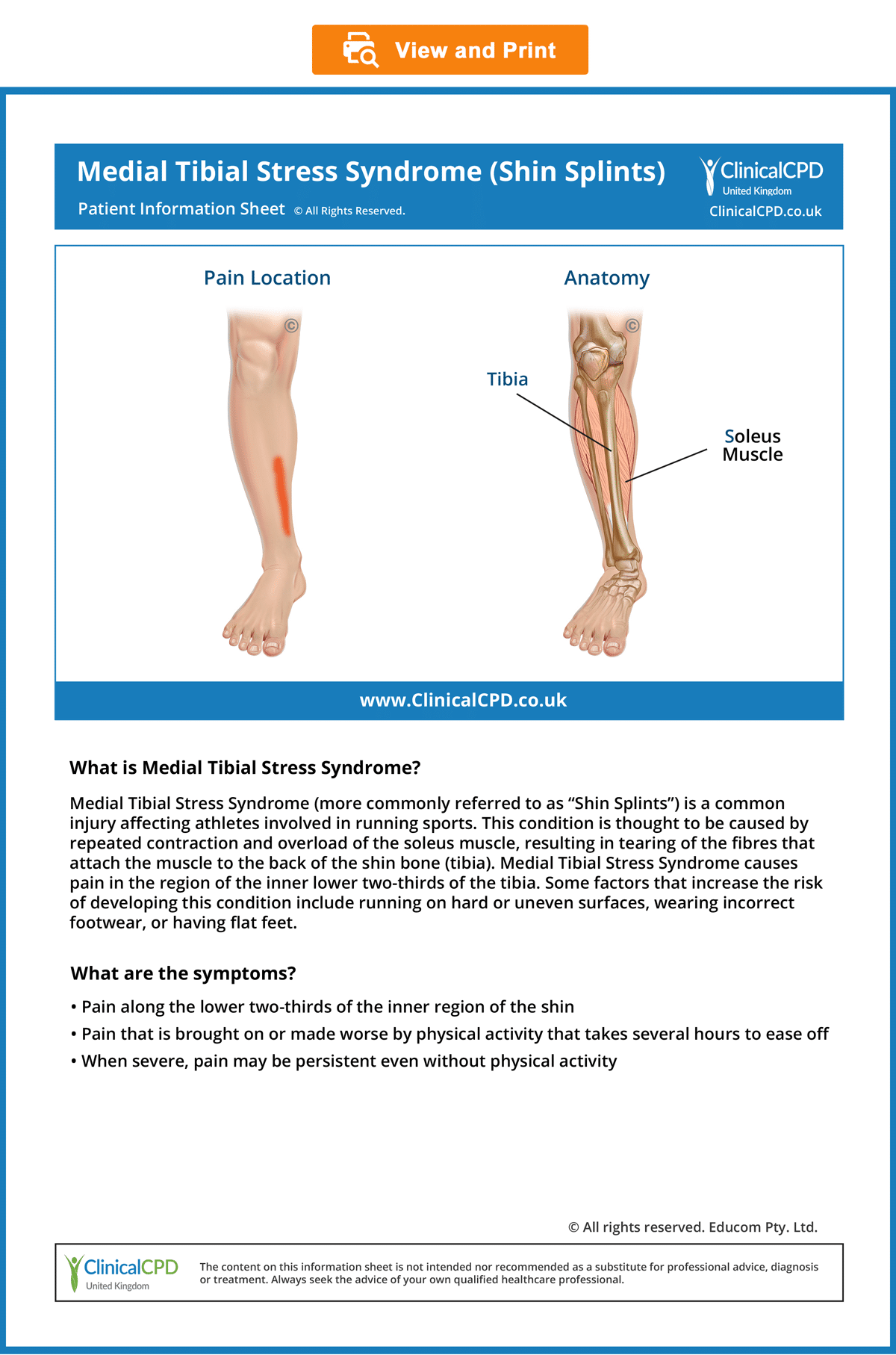
Patient Information Sheet
- Provide information to the patient about their condition to improve their understanding and enhance compliance (see the downloadable ready-to-use Patient Information Sheet below).
- In our experience, patients who are well informed about their condition are more likely to comply with the recommended management strategy, achieve good outcomes, become loyal patients, and recommend their family and friends to seek treatment.
- To view, download, or print the Patient Information Sheet, simply click on the image below.
© Educom Pty. Ltd. All Rights Reserved.
Disclaimer: The Clinical CPD™ website (including the text, graphics and videos that appear on the clinicalcpd.co.uk) are designed to offer users general health information for educational purposes only. The general health information furnished on this site is not intended to replace personal consultation with a qualified healthcare professional. You must always seek the advice of a healthcare professional for questions related to your disease, disease symptoms, and appropriate therapeutic treatments.
Copyright © Educom Pty Ltd: All material on this website (including the text, graphics, videos and downloadable files) are owned by or licensed to Educom Pty Ltd and is subject to copyright and other intellectual property rights under international conventions.
Quiz: This concludes the learning material for this unit. You may review the material or take the multiple-choice quiz for this unit now or at a later time. The quiz for this unit must be completed before you can access the next unit in this course. You can attempt the quiz as many times as you need to achieve a pass mark of at least 60%.
To take the quiz click the button below.